- Received April 29, 2024
- Accepted June 03, 2024
- Publication July 20, 2024
- Visibility 3 Views
- Downloads 1 Downloads
- DOI 10.18231/j.idjsr.2024.017
-
CrossMark

- Citation
Digital radiographic evaluation of obturation quality in primary molars using two obturation techniques: An in vivo study
- Author Details:
-
 Syeda Najeya Banu *
Syeda Najeya Banu *
-
Sunil Raj N
-
Anitha Anand
-
Nandan N
-
Soundarya V
-
Supriya P R
Introduction
Primary teeth are essential for optimum oral health. They should be maintained until their normal exfoliation time to provide proper guidance for the eruption of permanent teeth, to maintain arch length, for optimal mastication, and to enhance aesthetics and phonetics. Once the tooth becomes carious and involves pulp tissue, causing necrosis of pulpal soft tissue, pulpectomy becomes the treatment of choice in primary teeth to preserve the arch integrity, as the natural tooth is the best space maintainer.[1] One of the main objectives of paediatric dentistry is to preserve the integrity of the primary teeth in the oral cavity.
The success rate of pulpectomy depends on good case selection, biomechanical preparation, the type of obturating material, and the obturating technique used to achieve an excellent hermetic seal with minimum voids.[2]
Root canal obturation aims to eliminate any portals of entry between the root canal and the periodontium. The intricate root canal systems of primary teeth thus determine the outcome of treatment, which has an impact on the success of root canal therapy. Thus the success rate of endodontic therapy is significantly influenced by two factors: the obturating technique and the obturating material.[3], [4]
An ideal filling technique should satisfy the complete filling of the canal without overfill and with minimal or no voids. The endodontic pressure syringe, amalgam plugger, disposable syringe, reamers, machine syringe, pressure syringe, premixed syringe, cotton pellets, handheld lentulo spiral and motor driven lentulo spiral, Jiffy tube, endodontic plugger, tuberculin syringe, and most recently, the NaviTip are the most often used obturation techniques in primary teeth.[5], [6], [7], [8], [9]
The incremental filling technique is an extensively used obturation technique where we use an endodontic plugger corresponding to the size of the canal. The lentulo-spiral technique is the traditional and most frequently used obturating technique in primary teeth. Lentulo spiral is a root canal paste carrier and is either handheld or powered by a slow-speed handpiece.[10], [11] Despite the recent development of various innovative obturating procedures, none are ideal for the obturation of root canals in primary teeth.
Therefore, this randomised clinical trial was undertaken to evaluate the efficacy of motor-driven lentulospiral and incremental techniques for primary tooth obturation.
Materials and Methods
The current in vivo study was conducted in the Department of Pediatric and Preventive Dentistry. The Institutional Ethics Committee approved the study protocol.
The study included healthy and cooperative children aged four to seven years with at least one primary molar indicated for pulpectomy. Parents or guardians were requested to sign the consent form after the treatment procedure was explained.
Sample size estimation
The sample size was calculated at a 95% confidence interval and 80% power with an effect size of 0.05 and a critical chi-square value of 0.39 to compare two groups using G* Power 3.1.9.4. Thus, the total sample was 36.
The study involved 36 primary molars (8 maxillary and 28 mandibular) of children aged four to seven years who required pulpectomy based on inclusion and exclusion criteria.
Inclusion criteria
Young cooperative children with no history of systemic illness
Tooth with carious pulp exposure diagnosed as having irreversible pulpitis
No radiographic evidence of external/internal pathologic resorption
H/o spontaneous pain
Presence of interradicular/periapical radiolucency
Exclusion criteria
Children with special health care needs
Children with known allergies to zinc oxide eugenol (ZOE)
A non-restorable tooth
Tooth with more than 1/3 of root resorption
Mobility
Each tooth had to meet at least one of the aforementioned criteria. Selected teeth were randomly split into two groups of eighteen (n=18 each).
Group I- 18 primary molars obturated with hand plugger.
Group II-18 primary molars obturated with slow speed motor driven lentulo spiral.
A full mouth dental examination followed by a pre-operative radiograph of possible tooth indicated for pulpectomy was made.
Clinical procedure
All pulpectomy procedures were performed by a single investigator, with teeth isolated using a rubber dam after administering local anaesthesia.
Dental caries and overhanging enamel were removed with #330 high-speed bur. Access to the pulp was gained by sterile round bur, and the coronal pulp was amputated using a spoon excavator and irrigated with saline to view the canal orifice. Pulp tissue was extirpated from root canals using a barbed broach. The working length was maintained 1mm short of the radiographic apex using a #10 K file. Cleaning and shaping of the root canal was initiated with size 15K or Hedstorm file in pullback motion and then was sequentially increased up to size 35.Saline irrigation was carried out consistently following each instrumentation level. Root canals were dried with absorbent paper points before obturation.
Mixing of the ZOE
The obturating material used was ZOE (DEEPAK ENTERPRISE, MUMBAI INDIA) with consistencies as follows:
In Group I: one scoop of powder and two drops of liquid were mixed to a thicker consistency.
In Group II: two scoops of powder and two drops of liquid were mixed to a creamy consistency.
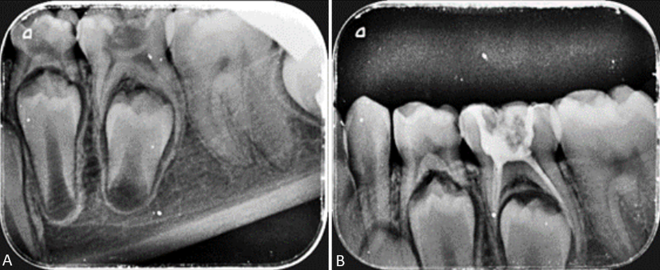
Obturation with hand plugger: [[Figure 2]]
An endodontic plugger (Mani Inc., Tokyo, Japan) with a rubber stop that matched the canal's size was used to obturate the tooth. A small increment of thickly mixed ZOE was carried into the root canal with an endodontic plugger. Cement was filled in three to four increments to fill the canal.
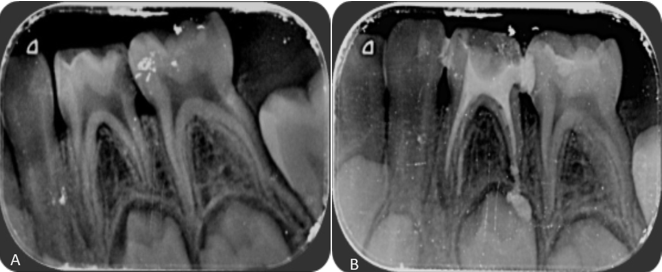
Obturation with slow-speed motor-driven lentulo-spiral: [[Figure 3]]
A 25mm lentulo-spiral (MANI, JAPAN), #25 mounted in a speed contra-angled handpiece (1000 rpm), was used to deliver the zinc oxide eugenol into root canals. A rubber stop was set 1mm short of the radiographic apex. Lentulo-spiral was placed into the root canals and rotated in a clockwise direction; simultaneously, a freshly mixed creamy mix of ZOE was carried into the canal using a cement spatula held near the rotating lentulo-spiral facilitating the uniform flow of material into the canals. When the backfill of the material into the pulp chamber occurred, the canal was assumed to be filled, and the lentulo-spiral was gently removed from the canal while still rotating.
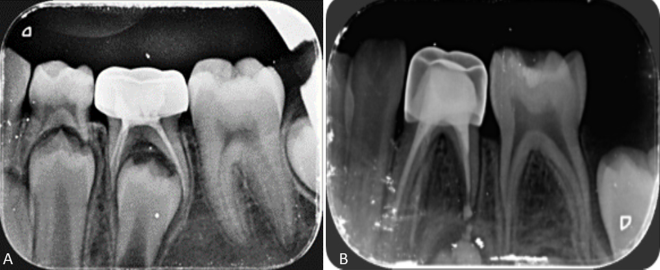
Following obturation, immediate post-operative radiographs were taken. The teeth were restored with glass ionomer cement (GC GOLD LABEL 9) followed by stainless steel crown (3M). [[Figure 4]]
Radiographic evaluation
The effectiveness of two obturating techniques was assessed using post-operative radiographs immediately after each obturation. Pre-operative and post-operative radiographs were taken with a PROMPT dental x-ray unit operating at 70kvp, 7mA. A photo-stimulable storage phosphor plate size 1 or 2 of the Vista scan system was used with an exposure of 0.03 sec and scanned in the proper scanner using the DSBWIN (Durr Dental AG, Beitigheim-Bissingen, Germany). Radiographic images obtained were scanned immediately after exposure and stored. Later, the radiographs were evaluated for quality of obturation by two examiners. If there was any ambiguity, a lower ranking was given.
Assessment of obturation techniques
Coll and Sadrian criteria (1996) was used for evaluating the quality of obturation and voids in obturated canals for radiographical comparison between the two techniques.
Apical seal
Under filling (score1): All the canals were filled more than 2 mm short of the radiographic apex
Optimal filling (score 2): One or more of the canals having obturation material ending at the radiographic apex or up to 2 mm short of the radiographic apex.$
Overfilling (score 3): Any canal showing obturation beyond the radiographic apex.[12]
Obturated canals were assessed for the presence or absence of voids.
The apical seal was measured in millimetres from the apical end of the canal filling material to the radiographic apex and scored as 1, 2, or 3. The highest score is regarded the overall quality of obturation for each tooth.
Statistical analysis
Statistical Package for Social Sciences [SPSS] for Windows, Version 22.0. Released in 2013. Armonk, NY: IBM Corp. was used to perform statistical analyses.
Descriptive statistics
Descriptive analysis expresses all explanatory and outcome variables in frequency and proportions.
Inferential statistics
The Chi-Square test was used to compare the tooth treated, the presence of voids, and the quality of obturation between groups. Cohen's Kappa Statistics was used to assess inter-observer variability in the Quality of Obturation in Groups 1 and 2. The level of significance [P-Value] was set at P<0.05.
Results
|
Comparison of Quality of Obturation between 2 groups using Chi-Square Test |
||||||
|
Variable |
Category |
Group 1 |
Group 2 |
p-value |
||
|
n |
% |
n |
% |
|||
|
Quality of Obturation |
Under filling |
2 |
11.1% |
0 |
0.0% |
0.04* |
|
Optimal filling |
12 |
66.7% |
8 |
44.4% |
||
|
Over filling |
4 |
22.2% |
10 |
55.6% |
Interpretation of [Table 1]
In terms of quality of obturation,
Under filled canals were more in group 1 (11.1%)
Group 1 (incremental filling technique) demonstrated a greater number of optimal filling, 12 (66.7%), compared to Group 2 (motor-driven lentulospiral technique), which had 8 (44.4%) optimal filling.
With respect to overfilling, more overfilled canals were found in group 2 (55.6%) when compared with group 1 (22.2%).
The results obtained were found to be statistically significant (p= 0.04).
Interpretation of [Table 2]
|
Comparison of Presence of Voids between 2 Groups Using Chi-Square Test |
||||||
|
Variable |
Category |
Group 1 |
Group 2 |
p-value |
||
|
n |
% |
n |
% |
|||
|
Voids |
Present |
12 |
66.7% |
12 |
66.7% |
1.00 |
|
Absent |
6 |
33.3% |
6 |
33.3% |
In this study, the presence of voids in the canals was a constant finding. No statistically significant difference (P=1.00) was observed when both techniques were assessed with regard to the presence of voids.
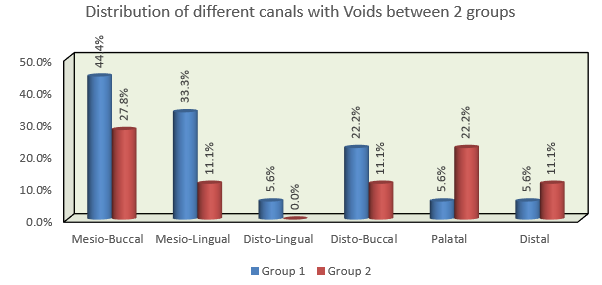
Comparing mesiobuccal root canals in groups 1 and 2, the percentage of voids was approximately 44.4% and 27.6% greater, respectively, than in the other canals. However, there were no statistically significant results.[Figure 1]
Discussion
A root canal treatment aims to efficiently and tightly fill the canal without overfilling it, leaving as little space as possible. Very few studies are available that evaluate the most commonly used incremental technique for filling the canal. Therefore, this study was conducted to compare the effectiveness of motor-driven lentulospiral with incremental techniques.
In our current study, the incremental approach (Group I) produced the most favourable outcomes, with the highest ideal fill rate, 66.7%. The motor-driven lentulo spiral approach (Group II) achieved an optimal filling rate of 44.4%, which was statistically significant (p<0.05) as shown in [[Table 1]]. The present study's findings are comparable to the previous research by Dandashi et al [13] that showed the best apical seal with a hand plugger to fill ZOE compared to a syringe system.
In the present study, the motor-driven lentulospiral approach (Group II) exhibited a considerably greater percentage of over-filled canals (55.6%), and none of the canals filled using this method was under-filled.
The flexibility of the lentulo spiral was attributed to these findings. Aminabadi et al[4] obtained similar results in a comprehensive review and meta-analysis, with motor-driven lentulo spirals accounting for 23.3% of overfilled obturation. Thus, overfilled obturation is a major drawback of the lentulo spiral technique, also influenced by factors like pathological lesions, thin dentinal walls, resorption, canal anatomy, operator skills, and the consistency of the obturating material. [11]
The present outcome was in contrast with studies done by Singh et al [14] Staehle et al [7] and Anika S et al [9] which revealed that motor-driven lentulo spiral system revealed significantly better results when compared to hand instruments. Upon evaluating individual canals, no statistically significant difference was observed.
Chandrasekhar et al compared three spiral technique with incremental technique. The authors concluded that the lentulo spiral approach was more successful in filling root canals, with maximum amount of optimal filled canals. Bidirectional spiral exhibited equivalent success. The incremental technique exhibited the least number of optimal fills. [10]
In the current study, ZOE paste was used as the obturating material considering its ubiquitous use and cost-effectiveness, and most investigators have utilized ZOE for evaluation. [2]
The vast contrariety of opinions among the present study and the previous studies could be due to the following reasons:
Type of material
Operator's skill and experience
The different consistencies of ZOE
Radiographs are minimally invasive and inexpensive to evaluate the quality of treatment in in-vivo studies. Studies have shown no difference between digital images, conventional radiographs, and digitally zoomed images for void detection in root canal fillings. Hence, we used a digital radiographic technique to compare two different root canal filling methods. [3], [15]
Comparing both techniques for voids [[Table 2]], the present study showed about 66.7% of cases with voids, which was not statistically significant (p=1.00). Voids were inevitable in both techniques. In the present study, voids were analysed using digital radiographs, which produced two-dimensional shadows, making it challenging to determine the exact position and amount of voids present, which may be a limitation of our study. Dandashi et al., in their in vitro study, analysed voids using multiple views (lateral and anterior/posterior radiographs), which was not feasible in our in vivo study. [15]
The presence of voids in the obturation can contribute to paths for leakage and increase the risk of microbe and toxin retention, resulting in post-treatment failure. Factors influencing the location and size of the voids include the type, viscosity, and consistency of the paste, the technique used, and operator skill and experience. [3], [15]
The lentulo spiral, two sizes smaller than the master Hedstorm /K-file and one millimetre shorter in working length, was used to carry ZOE to the root canals of primary teeth. Implementing this method revealed no broken lentulo spirals. To minimize the risk of fracture, use the lentulo spiral 1 to 2 sizes smaller than the master apical file. This allows ample space for the lentulo spiral to spin, and there will be less chance of it becoming engaged in the narrow root canal. This is a key to the safe use of the lentulo spiral.[3]
Limitations
In the present study, two-dimensional digital radiography was used to assess the obturation quality and voids' presence. Three-dimensional images would have given a better assessment of these parameters.
As this was an in vivo study, the sample size might be small to generalize the results to a larger population.
The current classification of under fill v/s optimal fill is confusing, and a canal-specific classification (KEDOO classification) [16] is needed to address these limitations and to improve the specificity and efficacy.
Conclusion
There was no statistically significant difference in void frequency between pluggers and lentulospirals (P = 1). However, based on the current in vivo study results, it can be inferred that the incremental approach was effective, providing a greater number of optimally filled canals than the slow-speed motor-driven lentulospiral.
As a result, for optimal primary tooth obturation, the traditional incremental procedure may be preferable to newer, more expensive, technique-sensitive obturation techniques. However, further randomized clinical studies comparing these two techniques with larger sample sizes and longer follow-up periods are needed to substantiate the results of the present study.
Source of Funding
None.
Conflict of Interest
None.
References
- R Kalaskar, H Badhe, N Thosar. Comparative Evaluation of Effectiveness of Premixed Syringe and Incremental Technique as a Root Canal Obturating Technique in Primary Mandibular Second Molar-A Randomized Clinical Trial. Ann Romanian Soc Cell Biol 2021. [Google Scholar]
- S Rajasekhar, SK Mallineni, S Nuvvula. Comparative evaluation of three obturation systems in primary molars–A randomized clinical trial. J Indian Soc Pedod Prev Dent 2019. [Google Scholar]
- J Ellanajermiah, A Rao, N Srikant, A Rao, BS Suprabha. Comparative Evaluation of Three Obturating Techniques in Primary Molars: An in Vivo Study. J Clin Pediatr Dent 2019. [Google Scholar]
- NA Aminabadi, NA Aminabadi, Z Jamali, S Shirazi. Primary tooth pulpectomy overfilling by different placement techniques: A systematic review and meta-analysis. J Dent Res Dent Clin Dent Prospects 2020. [Google Scholar]
- M Guelmann, M Mceachern, C Turner. Pulpectomies in primary incisors using three delivery systems: an in vitro study. J Clin Pediatr Dent 2004. [Google Scholar]
- SR Aylard, R Johnson. Assessment of filling techniques for primary teeth. Pediatr Dent 1987. [Google Scholar]
- HJ Staehie, C Thomä, HP Müller. Comparative in vitro investigation of different methods for temporary root canal filling with aqueous suspensions of calcium hydroxide. Endod Dent Traumatol 1997. [Google Scholar]
- MB Dandashi, MM Nazif, T Zullo, MA Elliott, LG Schneider, M Czonstkowsky. An in vitro comparison of three endodontic techniques for primary incisors. Pediatric Dent 1993. [Google Scholar]
- SA Anika, J Nessa, AZ Shikder, NM Joty, MM Galib, S Islam. A Comparative Evaluation of Obturation Techniques in Primary Molars between Incremental filling technique and Lentulo Spiral Technique. 2023. [Google Scholar]
- S Chandrasekhar, MG Prasad, AN Radhakrishna, K Saujanya, NV Raviteja, B Deepthi. A comparative In vivo efficacy of three spiral techniques versus incremental technique in obturating primary teeth. 2018. [Google Scholar]
- M Khubchandani, MS Baliga, SS Rawlani, S Rawlani, KM Khubchandani, N Thosar. Comparative evaluation of different obturation techniques in primary molars: An in vivo study. Eur J General Dent 2017. [Google Scholar]
- JA Coll, R Sadrian. Predicting pulpectomy success and its relationship to exfoliation and succedaneous dentition. Pediatr Dent 1996. [Google Scholar]
- MB Dandashi, MM Nazif, T Zullo, MA Elliott, LG Schneider, M Czonstkowsky. An in vitro comparison of three endodontic techniques for primary incisors. Pediatr Dent 1993. [Google Scholar]
- R Singh, S Chaudhary, N Manuja, TR Chaitra, AA Sinha. Evaluation of different root canal obturation methods in primary teeth using cone beam computerized tomography. J Clin Pediatr Dent 2015. [Google Scholar]
- K Vashista, M Sandhu, V Sachdev. Comparative evaluation of obturating techniques in primary teeth: An in vivo study. Int J Clin Pediatr Dent 2015. [Google Scholar]
- G Jeevanandan, L Govindaraju, N Kotian, PC Maganur, N Marwah, S Vishwanathaiah. A New Criteria to Assess Quality of Obturation in Primary Teeth: KEDOO Classification. Int J Clin Pediatr Dent 2023. [Google Scholar]
- Introduction
- Materials and Methods
- Sample size estimation
- Inclusion criteria
- Exclusion criteria
- Clinical procedure
- Obturation with hand plugger: [[Figure 2]]
- Obturation with slow-speed motor-driven lentulo-spiral: [[Figure 3]]
- Radiographic evaluation
- Assessment of obturation techniques
- Statistical analysis
- Descriptive statistics
- Inferential statistics
- Results
- Discussion
- Limitations
- Conclusion
- Source of Funding
- Conflict of Interest